Author: Dr. Steffy Mariyam Reji, (Specialist Dermatologist – Wellkins Medical Centre)
You may not know the medical name for it but the chances are you have seen it or felt it at some point, either on yourself or on someone close to you. Small rough bumps on the upper arms, thighs or cheeks that look a little like goosebumps that never quite go away. Skin that feels like sandpaper to the touch. A texture that moisturizer softens temporarily but never fully resolves.
This is keratosis pilaris, commonly referred to as chicken skin, and it is one of the most frequently asked about skin conditions in the dermatology clinic at Wellkins Medical Centre in Doha. It affects an estimated 40 percent of adults and up to 80 percent of adolescents to some degree, making it one of the most prevalent skin conditions globally, yet it remains widely misunderstood, frequently mistreated and almost universally underdiagnosed.
The good news is straightforward: keratosis pilaris is entirely harmless. It is not contagious, not painful in the vast majority of cases and not a sign of poor hygiene or poor health. But for many people it is a source of genuine self-consciousness, particularly in Qatar’s warm climate where arms and legs are more frequently exposed and where the condition’s characteristic rough texture is difficult to ignore. Understanding what it is, why it happens and what actually works to manage it is where the story of effective treatment begins.
Keratosis pilaris is the condition I see most frequently dismissed before patients arrive at the clinic, either because they have been told it is just dry skin or because they have tried a regular moisturizer without improvement and concluded that nothing will help. Neither is accurate. Keratosis pilaris is a specific follicular condition that requires specific treatment ingredients to improve. The right combination of exfoliation, barrier support and targeted active ingredients produces genuine and visible improvement in the vast majority of cases. It requires consistency rather than complexity, and the results when patients commit to the right routine are often significantly better than they expected.
People Also Ask
What is chicken skin (keratosis pilaris)?
Keratosis pilaris is a common benign skin condition in which keratin, the protein that forms the outer layer of skin, builds up inside the hair follicle openings and forms small rough plugs. These plugs produce the characteristic bumps that give the skin a rough sandpaper-like texture, most commonly on the upper arms, thighs, buttocks and in some people the cheeks and jawline. The condition is entirely harmless, not contagious and not related to hygiene. It affects people of all skin tones and is particularly prevalent in children and adolescents though it frequently persists into adulthood.
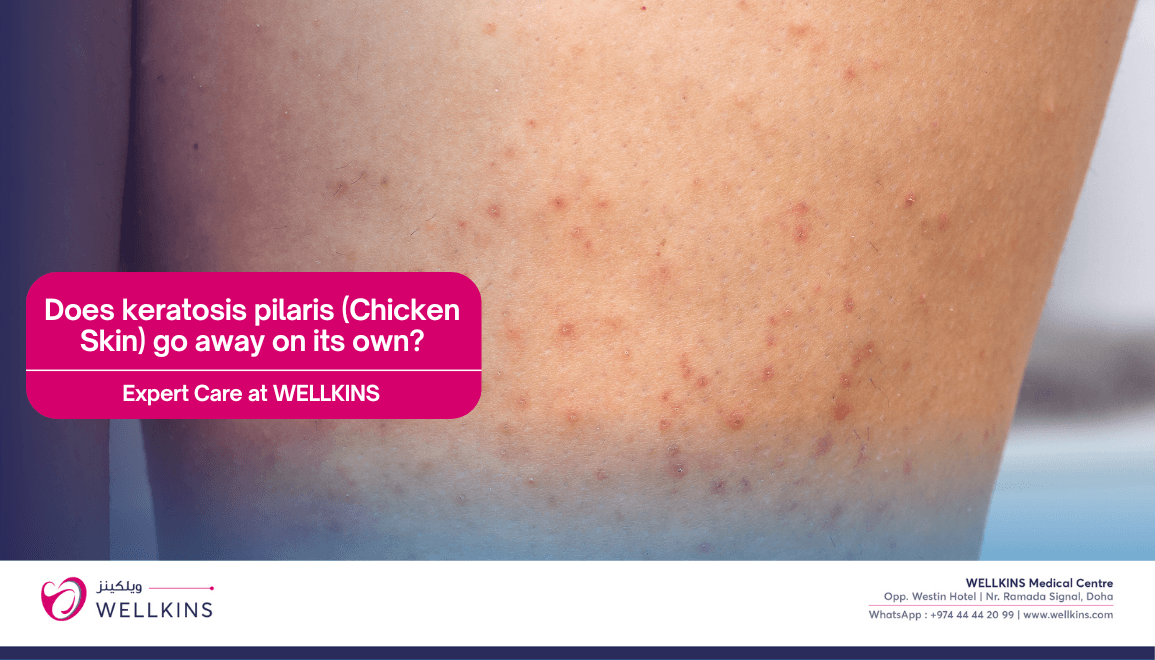
Does keratosis pilaris go away on its own?
For some people keratosis pilaris improves naturally with age, often becoming less pronounced in the late twenties and beyond as the skin’s rate of keratin production changes. However it does not resolve spontaneously for everyone and for many adults it persists throughout their lives with seasonal variation. The condition tends to worsen during winter months and in dry air-conditioned environments due to the drying effect on the skin, which is particularly relevant in Qatar where air conditioning is used intensively year-round. With appropriate management most patients achieve significant and sustained improvement.
What makes keratosis pilaris worse?
Dryness is the most consistent trigger for worsening keratosis pilaris as it increases the rate of keratin accumulation and makes the bumps more prominent and more rough to the touch. In Qatar, the combination of intense air conditioning, low indoor humidity, high outdoor UV exposure and the frequent hot showers that the climate encourages all contribute to the skin dryness that exacerbates the condition. Aggressive physical scrubbing, harsh soaps that strip the skin barrier and certain body washes with high alcohol content can also worsen the condition by irritating the follicles and increasing inflammation around the bumps.
What ingredients actually treat keratosis pilaris?
The most evidence-supported ingredients for keratosis pilaris are chemical exfoliants including urea, lactic acid, glycolic acid and salicylic acid which dissolve the keratin plugs rather than scratching at them, and emollients that reinforce the skin barrier and prevent the dryness that allows plugs to reform. Retinoids including retinol and prescription tretinoin promote cell turnover and reduce follicular plugging over time. Regular consistent use of the right combination produces the most reliable results. A dermatologist assessment identifies which ingredients and concentrations are appropriate for your specific skin type and condition severity.

What Is Keratosis Pilaris (Chicken Skin)?

Keratosis pilaris is a follicular skin condition caused by the overproduction and accumulation of keratin within the opening of individual hair follicles. Keratin is the fibrous structural protein that forms the outer protective layer of skin, nails and hair. In keratosis pilaris the body produces excess keratin that plugs the follicle opening rather than shedding normally as part of the skin’s natural renewal cycle.
These keratin plugs form small raised bumps on the skin surface that are typically flesh-coloured, white or very slightly red, clustered around the hair follicle and surrounded by skin that may have a mild pinkish or reddish tint due to mild inflammation around the blocked follicle. The bumps are most commonly distributed across the outer upper arms and are the reason the condition is so often noticed on the backs of the arms specifically. The anterior thighs, buttocks and in younger children and some adults the cheeks and jawline are also commonly affected areas.
The condition is not an infection. It is not contagious. It is not related to cleanliness or hygiene and it is not caused by diet in most people. It is a genetically influenced variation in how the skin processes and sheds keratin and its prevalence within families is significant. If one parent has keratosis pilaris the chance of their children developing it is considerably higher than in the general population.
Who Gets Keratosis Pilaris?
Keratosis pilaris is remarkably common. It affects an estimated 40 percent of the adult population and up to 80 percent of adolescents, making it one of the most widespread skin conditions seen in dermatology practice. Despite this prevalence it is significantly underrecognized, with most people either not knowing the name of the condition they have or having been told simply that their skin is dry.
Several factors increase the likelihood of developing or worsening keratosis pilaris.
- Genetics: A family history of keratosis pilaris is the strongest risk factor. The condition follows an autosomal dominant inheritance pattern meaning a child of an affected parent has a significant likelihood of developing it themselves.
- Dry Skin: People with naturally drier skin types have a higher prevalence and more pronounced presentation of keratosis pilaris. The condition worsens significantly in low-humidity environments and during periods of increased skin dryness.
- Atopic Conditions: Keratosis pilaris is strongly associated with atopic dermatitis, eczema and allergic conditions. People with these conditions are significantly more likely to develop keratosis pilaris and often manage both concurrently.
- Adolescence and Childhood: The condition is most prevalent during childhood and adolescence, often becoming apparent in early childhood and tending to be most pronounced during puberty before improving somewhat in many people in their late twenties.
- Qatar-Specific Factors: The intensive year-round air conditioning in Qatar’s homes, offices and shopping malls creates a chronically low-humidity indoor environment that consistently strips moisture from the skin. This environmental dryness is one of the most significant exacerbating factors for keratosis pilaris in Doha’s population and means that patients here often experience more pronounced and more persistent symptoms than they might in a more humid climate.
Recognizing Keratosis Pilaris: What It Looks and Feels Like
The appearance and texture of keratosis pilaris are distinctive enough that most cases can be identified on clinical examination without any special investigations.
- Small Rough Bumps: The most characteristic feature is small firm bumps clustered around hair follicle openings, giving the skin a texture that is commonly compared to sandpaper, goosebumps that do not resolve or the surface of a plucked chicken, which is the origin of the common name chicken skin.
- Colouration: The bumps themselves are typically flesh-coloured or white. The skin surrounding individual bumps may have a reddish or pinkish discoloration from the mild follicular inflammation around the plug, which in fair skin tones gives the affected area a slightly flushed appearance.
- Distribution: Most commonly the outer upper arms. Also frequently the anterior thighs, buttocks and in children and some adults the cheeks and jawline. The condition is almost never seen on the palms, soles or mucous membranes.
- Texture Without Tenderness: The affected skin is rough to the touch but not usually painful. Some people experience mild itching particularly when the skin is very dry. Significant pain or tenderness would suggest a secondary complication including folliculitis that warrants separate assessment.
- Seasonal Variation: Most people with keratosis pilaris notice it worsens in winter and in dry conditions and improves somewhat in the more humid summer months, though in Qatar the dominance of air conditioning means this seasonal improvement is often less pronounced than patients experience when they travel to more humid environments.
What Actually Works: Treatment Options for Keratosis Pilaris
Keratosis pilaris cannot be permanently cured but it can be very effectively managed with the right combination of ingredients and consistent application. The goal of treatment is to dissolve the keratin plugs, support the skin barrier to prevent their reformation and reduce the surrounding inflammation where it is present.
- Chemical Exfoliants: This is the most important category of treatment ingredient for keratosis pilaris and the one that most patients have not tried when they arrive at the clinic. Chemical exfoliants including urea at concentrations of ten to thirty percent, lactic acid, glycolic acid and salicylic acid work by dissolving the bonds holding the keratin plug together rather than physically scrubbing at it. Physical scrubbing can actually worsen the condition by irritating the follicle and increasing inflammation. A urea-based body lotion or an AHA body wash used consistently is typically the most effective foundation of a keratosis pilaris skincare routine.
- Emollients and Barrier Repair: Keeping the skin well moisturized is essential both for reducing the prominence of existing bumps and for preventing new plugs from forming in dry skin. Thick emollient creams or ointments containing ingredients including ceramides, shea butter or glycerin applied immediately after bathing while the skin is still slightly damp produce the most effective hydration. In Qatar’s air-conditioned environment daily emollient application is particularly important.
- Retinoids: Topical retinoids including over-the-counter retinol and prescription tretinoin promote accelerated skin cell turnover, which reduces the rate at which keratin accumulates in the follicle and helps existing plugs clear more quickly. Retinoids are particularly useful for patients with more persistent or more inflamed presentations. They are used in the evening and always alongside consistent sun protection given the increased photosensitivity they produce.
- In-Clinic Treatments: For patients whose keratosis pilaris has not responded adequately to topical management or who have significant post-inflammatory discoloration alongside the bumps, in-clinic options at Wellkins Dermatology include professional chemical exfoliation treatments and laser or light-based therapies that target both the follicular plugging and the surrounding redness. These are discussed and tailored based on individual skin type and presentation.
- What to Avoid: Harsh physical scrubs, rough loofahs and aggressive rubbing during and after bathing all worsen keratosis pilaris by irritating the follicles and increasing inflammation. Very hot showers strip the skin barrier and worsen dryness. Fragranced body washes and products with high alcohol content also impair barrier function and should be replaced with gentle unscented alternatives.
Building a Keratosis Pilaris Skincare Routine for Qatar’s Climate
The principles of an effective keratosis pilaris skincare routine are straightforward but the specific products and application practices matter considerably in Qatar’s environment.
- Shower in Lukewarm Rather Than Hot Water: Hot water strips the skin’s natural oils and dramatically worsens the dryness that drives keratosis pilaris. Lukewarm showers of no more than ten minutes preserve the skin barrier while still cleansing effectively.
- Use a Gentle Soap-Free Cleanser on Affected Areas: Standard soap bars and heavily fragranced body washes are alkaline and strip the skin barrier. Switching to a gentle pH-balanced or soap-free wash reduces the barrier damage that worsens keratosis pilaris with every shower.
- Apply a Urea or AHA Body Lotion Immediately After Bathing: Pat the skin gently dry and apply a chemical exfoliant body lotion while the skin is still slightly damp. This is the step that most consistently produces visible improvement in texture when maintained over four to eight weeks.
- Use a Richer Emollient at Night: A thicker cream or ointment applied to affected areas at night allows longer contact time with the skin and produces deeper hydration than a lotion applied in the morning before clothing is put on.
- Use Sun Protection on Exposed Affected Areas: Sun exposure worsens the redness and post-inflammatory discoloration associated with keratosis pilaris. Daily broad-spectrum SPF applied to arms and legs before outdoor exposure in Qatar’s high-UV environment is a practical and important part of managing the visible redness alongside the texture.
When to See a Dermatologist at Wellkins

Keratosis pilaris is a condition that many people manage independently for years with varying success. A dermatologist consultation at Wellkins Medical Centre is particularly worthwhile if any of the following apply.
- You have been using a standard moisturizer without improvement and are not sure which specific ingredients your skin actually needs.
- The affected areas are significantly red or inflamed alongside the rough texture, suggesting active follicular inflammation that may benefit from prescription treatment.
- You have post-inflammatory discoloration, either darker or lighter patches, remaining after the bumps in areas that have been scratched or irritated over time.
- The condition is affecting your confidence or your willingness to wear certain clothing, particularly relevant in Qatar’s social and outdoor environment.
- You are unsure whether what you have is keratosis pilaris or another follicular condition including milia, folliculitis or a different form of dermatitis that would require different management.
Chicken skin has a name, a clear mechanism and a genuinely effective treatment pathway. It is not something to simply live with when the right guidance makes a visible difference. If your skin’s texture has been frustrating you, this is exactly the kind of problem that a targeted dermatology consultation at Wellkins resolves.
To book an appointment with Dr. Steffy Mariyam Reji at Wellkins Medical Centre: https://wellkins.com/drsteffy
To know more about the Orthopedic services at Wellkins Medical Centre: https://wellkins.com/dermatology