Author: Dr. Asha Anne Jacob, ( Consultant Ophthalmologist – WELLKINS Medical Centre )
Qatar has one of the highest rates of diabetes in the world. Estimates consistently place the prevalence of type 2 diabetes among Qatar’s adult population at among the highest globally, and when prediabetes is included the numbers are even more striking. Behind this statistic is a quieter and far less discussed consequence that unfolds gradually and silently inside the eyes of people living with the condition every day.
Diabetic eye disease is the leading cause of preventable blindness among working-age adults worldwide. In Qatar, where diabetes rates are so elevated, the burden of vision-threatening diabetic eye complications is correspondingly significant. And yet the majority of patients who develop diabetic eye disease do not know it is happening until it has already progressed to a stage where treatment becomes substantially more complex and the outcomes considerably less certain.
This is the central and most important truth about diabetic eye disease: it gives almost no warning before it has caused damage. The eyes do not hurt. Vision may remain seemingly normal for years. By the time a patient notices something is wrong, an opportunity for simpler and more effective intervention has very often already passed.
Of all the complications of diabetes, eye disease is the one I find patients are least prepared for when they first hear about it. They know about kidney problems and nerve damage and heart disease. But they are genuinely surprised when I explain that their retina has been quietly changing for years because their blood sugar has not been well controlled. The damage is invisible until it is not, and by then we are managing a much harder problem than we would have been at an earlier stage. A diabetic eye examination is not optional and it is not something to delay until vision changes. It is the single most important thing a person with diabetes can do for their long-term sight.
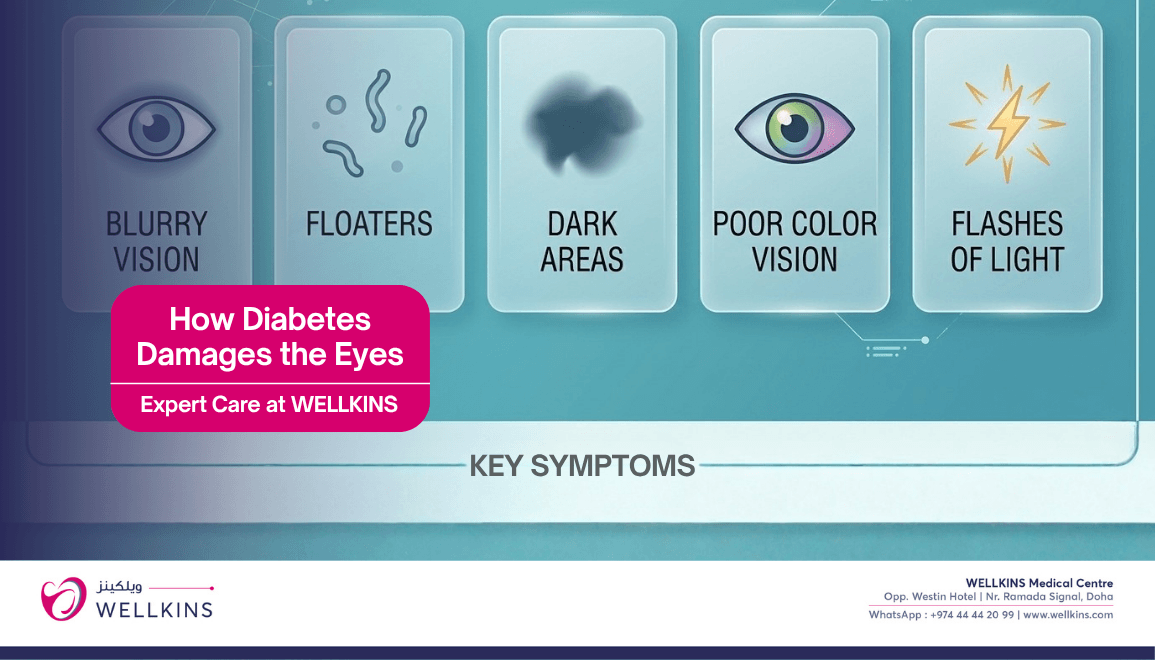
How Diabetes Damages the Eyes
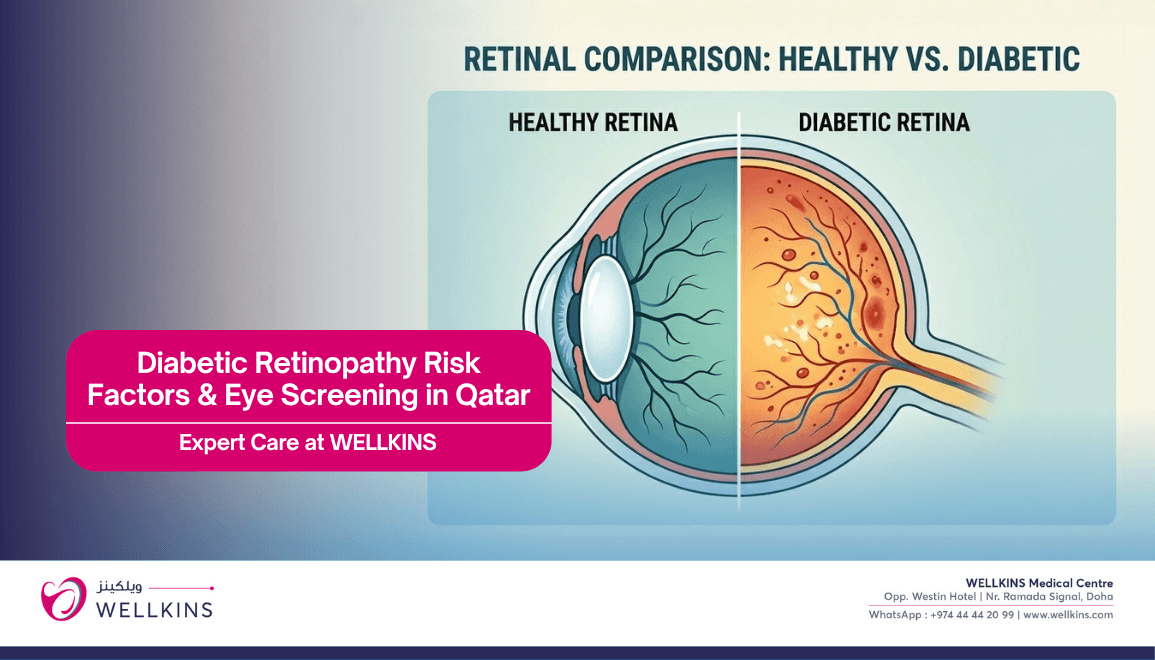
Understanding why diabetes affects the eyes begins with the retina, the thin layer of light-sensitive tissue at the back of the eye that converts visual information into signals sent to the brain. The retina is one of the most metabolically active and most vascularly dense tissues in the entire body. It depends entirely on a fine network of tiny blood vessels to deliver the oxygen and nutrients it needs to function.
Chronically elevated blood glucose damages these small blood vessels throughout the body, but the retinal vessels are particularly vulnerable. High glucose levels cause the walls of these vessels to weaken, become leaky and develop abnormal areas of dilation called microaneurysms. As the disease progresses, some vessels close off entirely, depriving areas of the retina of their blood supply. The retina, detecting this ischemia, responds by stimulating the growth of new blood vessels in a process called neovascularization. These new vessels are structurally fragile and prone to bleeding. They can grow across the retinal surface and into the vitreous gel of the eye, and when they bleed or contract they can cause devastating and rapid visual loss.
This entire process, from the first microscopic vessel changes to severe sight-threatening complications, can unfold over years with no symptoms that the patient can detect independently.
The Spectrum of Diabetic Eye Disease
Diabetic eye disease is not a single condition. It encompasses several distinct but interrelated conditions that affect different structures of the eye in different ways and at different stages of the disease process.
1. Diabetic Retinopathy
Diabetic retinopathy is the most common and most clinically significant diabetic eye condition. It is staged according to severity and the staging system directly guides treatment decisions.
- Non-Proliferative Diabetic Retinopathy (NPDR): The earliest stage, characterized by microaneurysms, small retinal hemorrhages, hard exudates from leaking lipids and cotton wool spots from nerve fiber layer infarcts. At this stage the patient typically has no symptoms and vision may be entirely normal. NPDR is further divided into mild, moderate and severe categories based on the extent of these changes.
- Proliferative Diabetic Retinopathy (PDR): The advanced stage defined by the growth of new, abnormal blood vessels on the retinal surface or optic disc. These vessels bleed easily into the vitreous, causing sudden vision loss, and can lead to tractional retinal detachment as fibrous tissue contracts. Proliferative retinopathy is a sight-threatening emergency and requires urgent specialist intervention.
2. Diabetic Macular Oedema
The macula is the small central area of the retina responsible for the sharp, detailed vision used for reading, recognizing faces and driving. When the leaking retinal blood vessels of diabetic retinopathy allow fluid to accumulate within the macula, diabetic macular oedema develops. This is the most common cause of vision loss in diabetic patients and can occur at any stage of retinopathy, including in patients with relatively mild background changes.
- Symptoms: Blurring or distortion of central vision. Straight lines may appear wavy. Reading and near tasks become progressively more difficult. The peripheral vision is typically unaffected in the early stages, which is why patients may not notice the problem until the central vision loss is significant.
- Qatar Context: Given Qatar’s high rates of poorly controlled and late-diagnosed type 2 diabetes, diabetic macular oedema is among the most frequently encountered sight-threatening conditions in the ophthalmology clinic at Wellkins.
3. Diabetic Cataract
People with diabetes develop cataracts, clouding of the natural lens of the eye, at a significantly younger age and more rapidly than the general population. Chronically elevated glucose alters the metabolic environment of the lens, accelerating the oxidative changes that lead to clouding. Diabetic cataracts can develop in patients in their thirties and forties rather than the typical sixth and seventh decades of life.
- Impact: Progressive clouding of vision that affects both distance and near tasks. Glare from bright lights and oncoming headlights is a characteristic early complaint in patients developing cataract in Qatar’s intensely sunny environment.
4. Diabetic Glaucoma
Diabetes approximately doubles the risk of developing glaucoma, a condition characterized by damage to the optic nerve, most commonly from elevated intraocular pressure. Neovascular glaucoma, a particularly severe form caused by abnormal blood vessel growth in the drainage angle of the eye secondary to advanced diabetic retinopathy, can cause rapid and severe vision loss if not identified and treated urgently.
5. Diabetic Cranial Nerve Palsy
Less commonly, diabetes can damage the cranial nerves supplying the muscles that move the eye, causing sudden onset of double vision. This most commonly involves the third or sixth cranial nerve and typically resolves over weeks to months with good glycemic control, but requires urgent assessment to exclude other causes.
Who Is at Risk and Why Qatar’s Population Faces Elevated Danger
Every person with diabetes carries a risk of developing diabetic eye disease, but several factors significantly elevate that risk and are particularly prevalent in Qatar’s patient population.
- Duration of Diabetes: The single most powerful predictor of diabetic eye disease is how long a person has had diabetes. After twenty years of diabetes, the majority of patients with type 1 diabetes and a very significant proportion of those with type 2 diabetes will have some degree of retinopathy. In Qatar, where many patients are diagnosed late after years of undetected hyperglycemia, the effective duration of diabetes exposure is often longer than the official diagnosis date suggests.
- Poor Glycemic Control: HbA1c levels consistently above target are the most directly modifiable risk factor for the development and progression of diabetic eye disease. Each percentage point reduction in HbA1c produces a meaningful and well-documented reduction in the risk of retinopathy progression. Qatar’s population has among the highest rates of poorly controlled diabetes in the region.
- Hypertension: High blood pressure independently damages retinal blood vessels and significantly accelerates the progression of diabetic retinopathy when it coexists with diabetes. Hypertension is extremely prevalent in Qatar’s diabetic population.
- Dyslipidemia: Elevated cholesterol and triglyceride levels increase the risk of hard exudate formation within the macula and worsen diabetic macular oedema. Given the dietary patterns common in Qatar and across the Gulf, dyslipidemia in diabetic patients is a frequent and undertreated finding.
- Pregnancy: Pre-existing diabetic retinopathy can worsen significantly during pregnancy. Women with diabetes who are planning pregnancy or who are already pregnant should have retinal assessment as an urgent priority rather than a routine scheduling matter.
- Smoking: Smoking accelerates the microvascular damage of diabetes across all organ systems including the eye. In Qatar’s expat population, smoking rates among certain demographic groups remain significant.
- Late Diagnosis: Many patients in Qatar, particularly among the large expat working population, do not have access to regular preventive health monitoring. Diabetes is frequently diagnosed incidentally during a health check for another purpose, sometimes after a decade or more of subclinical hyperglycemia has already been silently damaging the retinal vessels.
The Silent Progression: Why Regular Screening Is Non-Negotiable
The defining clinical challenge of diabetic eye disease is its silence. This cannot be overstated.
A patient can have moderate non-proliferative diabetic retinopathy with significant vessel changes visible on a dilated fundus examination and have vision that tests at 6/6, normal, on a standard eye chart. There is no pain. There is no visual disturbance. There is nothing in the patient’s daily experience that suggests anything is wrong inside the eye. Yet the pathological process that will eventually threaten their vision is already well underway.
This is precisely why waiting for symptoms before seeking an eye examination is the single most dangerous mistake a person with diabetes can make about their ocular health.
The international guideline recommendations for diabetic eye screening are clear and consistent. Patients with type 1 diabetes should have their first dilated retinal examination within five years of diagnosis. Patients with type 2 diabetes should be examined at the time of diagnosis, as retinopathy may already be present given the typically long asymptomatic period before type 2 diabetes is identified. Following the initial examination, annual dilated fundus examinations are recommended for all diabetic patients as a minimum standard, with more frequent review for those with established retinopathy or other high-risk features.
In Qatar, where systemic health monitoring across the large and diverse working population is inconsistent, adherence to these screening intervals is significantly below what clinical guidelines recommend.
Diagnosis and Assessment at Wellkins Medical Centre
At Wellkins, diabetic eye assessment is a structured and thorough process that goes beyond a standard visual acuity check. The goal is not simply to confirm whether retinopathy is present but to stage it accurately, identify any macular involvement and provide a clear picture of the individual patient’s current risk and optimal review interval.
- Dilated Fundus Examination: The cornerstone of diabetic eye assessment. Pupil dilation with eye drops allows a comprehensive view of the peripheral retina, macula and optic disc that is not possible through an undilated pupil. This examination takes approximately thirty to forty-five minutes including the time needed for dilation and the examination itself.
- Intraocular Pressure Measurement: Screening for glaucoma, including the neovascular form associated with advanced diabetic retinopathy, is included in the comprehensive diabetic eye assessment.
- Visual Acuity and Refraction: Assessment of current visual function and the identification of any refractive changes associated with blood glucose fluctuation, a common and often overlooked phenomenon where acute changes in blood sugar alter the refractive index of the lens and cause temporary blurring of vision.
Treatment Options for Diabetic Eye Disease
Treatment of diabetic eye disease is determined by the specific diagnosis, the stage of disease and the individual patient’s clinical circumstances. The most effective intervention of all, however, remains prevention through rigorous systemic control.
- Optimizing Systemic Control: The most powerful treatment available for diabetic eye disease is keeping HbA1c, blood pressure and cholesterol within target ranges through medication, diet and lifestyle management. Studies have demonstrated that intensive glycemic control significantly reduces the incidence of retinopathy and slows its progression in patients who already have early changes. No ophthalmological intervention is as effective in the long term as a well-controlled HbA1c.
When to Book Your Diabetic Eye Examination at Wellkins
There is a specific group of people reading this for whom the answer to this question is: right now, today.
- You have been diagnosed with type 2 diabetes and have never had a dilated retinal examination.
- You have had diabetes for more than a year and your last eye examination was not a dilated fundus assessment by an ophthalmologist.
- You have noticed any change in your vision including blurring, distortion, floaters, flashing lights or sudden difficulty with reading or distance tasks.
- Your HbA1c has been consistently above target and you have not had an eye review in the past twelve months.
- You have diabetes alongside high blood pressure, high cholesterol or a long smoking history.
- You are pregnant with pre-existing diabetes or are planning pregnancy in the near future.
Sight lost to diabetic eye disease is largely preventable. The technology to detect it early is available. The treatments to slow or halt its progression are effective. The only thing that turns a manageable condition into an irreversible one is the absence of timely assessment.
Do not let that be your story. One examination could be the difference between preserving your vision and losing it. At Wellkins Medical Centre, that examination is available, thorough and performed with the expertise your eyes deserve.
To book an appointment at Wellkins Medical Centre: https://wellkins.com/visit